Clinical Case Practice for Medical Students: A Structured 15-Minute Framework

It is late evening after postings. A medical student opens a clinical case.
“52-year-old male with chest pain.”
The first diagnosis comes almost instantly. Myocardial infarction. The rest of the case becomes an effort to confirm that instinct.
The final answer matches.
There is relief.
But later, during discussion with a friend, a simple question comes up:
“Why were the other possibilities less likely?”
And the explanation feels incomplete.
This experience is common. Clinical case practice for medical students often begins this way. Not because students lack knowledge, but because clinical reasoning is rarely taught as a structured habit. Most of us learn it indirectly, by observing seniors or reading explanations after solving cases.
Over time, this creates a pattern. We become better at recognizing common presentations, but less confident when cases are slightly atypical.
Clinical case practice for medical students is often done with sincerity and effort. What is usually missing is a repeatable framework that trains how we think, not just what we conclude.
Even fifteen focused minutes a day, when structured well, can gradually build stronger diagnostic clarity through deliberate reflection.
In this article, we will explore a practical 15-minute framework that makes daily case practice more structured, more collaborative, and more aligned with how real clinical reasoning develops.
Why Clinical Case Practice Often Feels Unstructured
Most medical students do practice cases.
Some use textbooks.
Some use question banks.
Some discuss cases informally after rounds.
Yet many still feel that their clinical reasoning is unstable.
One day, a case feels straightforward.
The next day, a similar presentation feels confusing.
This inconsistency usually comes from three gaps.
1. Knowledge Without Process
Medical education provides large volumes of information. Pathophysiology, investigations, management protocols. But the step-by-step cognitive process of moving from symptom to structured differential diagnosis is rarely made explicit.
Students often know the content. What feels uncertain is the sequence of thinking.
What comes first?
What deserves priority?
When should a diagnosis move up or down the list?
Without a clear internal process, clinical case practice becomes reactive rather than deliberate.
2. Exposure Without Reflection
Solving more cases does increase exposure. However, exposure alone does not automatically improve reasoning.
If a student completes ten cases but does not pause to analyze:
- Why a diagnosis was considered early
- Why another was deprioritized
- Whether bias influenced the decision
The learning remains surface-level.
Reflection is what converts exposure into structured clinical reasoning practice.
3. Pattern Recognition Without Flexibility
Pattern recognition is essential in medicine. It develops naturally with repetition. However, if case practice is limited to matching symptoms to familiar patterns, students may struggle when presentations are incomplete or atypical.
Real patients rarely present in textbook format.
Clinical case practice for medical students must therefore train both:
- Pattern recognition
- Analytical reasoning
When only one is trained, confidence becomes fragile.
This is why many students feel they are “doing cases” but not steadily improving their diagnostic clarity.
The solution is not to solve more cases.
The solution is to introduce a small but consistent structure into each case encounter.
In the next section, we will build that structure step by step.
Why Random Case Solving Does Not Build Strong Clinical Reasoning
It is easy to assume that solving more cases automatically improves diagnostic ability.
If ten cases help, then fifty must help more.
In reality, improvement depends less on volume and more on how each case is approached.
Random case solving often creates three hidden problems.
1. Confirmation Over Exploration
When a case begins with a familiar symptom, the mind often moves quickly toward a likely diagnosis. From that point onward, the focus shifts to confirming that choice.
Investigations are interpreted through that lens.
Alternative possibilities receive less attention.
The case may still end with the correct answer. But the reasoning pathway remains narrow.
Over time, this reinforces a habit of premature closure, where the first reasonable diagnosis becomes the final one without adequate comparison.
This pattern is discussed in more depth in our article on common mistakes medical students make in clinical reasoning, which explores how subtle cognitive shortcuts shape decision making.
2. Answer Checking Instead of Reasoning Analysis
In many forms of clinical case practice for medical students, the workflow looks like this:
Read case → Choose diagnosis → Check answer → Read explanation → Move on
What is often missing is analysis of the thinking process itself.
- Why was one diagnosis prioritized?
- At what point did the differential list narrow?
- Which data point was decisive?
Without analyzing these steps, the student learns the conclusion but not the cognitive structure behind it.
Clinical reasoning improves when the process is examined, not only the result.
3. Inconsistent Cognitive Discipline
Some days, a student may carefully generate differentials. Other days, they may jump directly to a likely answer due to fatigue or time pressure.
Without a repeatable structure, the depth of reasoning varies from case to case.
Consistency is what builds durable diagnostic thinking. Randomness builds familiarity, but not reliability.
None of this suggests that solving cases is ineffective. It remains one of the most important tools in medical education.
However, without structure, clinical case practice becomes episodic rather than cumulative.
The goal is not to eliminate intuition. It is to discipline it.
In the next section, we will outline a simple 15-minute framework that introduces structure into every case, without increasing workload or complexity.
The 15-Minute Framework for Clinical Case Practice for Medical Students
This framework is not designed to slow you down.
It is designed to discipline your thinking.
Each step has a purpose.
Together, they create a repeatable cognitive structure.
The entire process can be completed in approximately fifteen focused minutes.
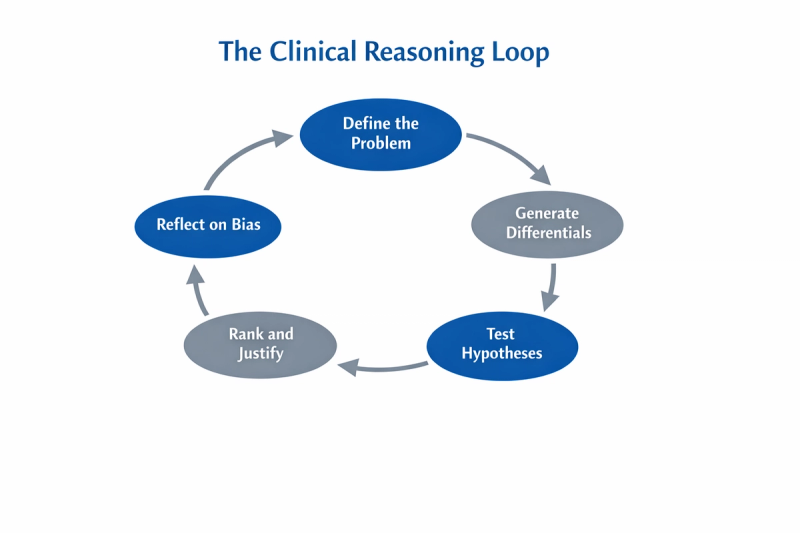
Overview of the 15-Minute Structure
Minute 1 to 3
Clarify the core problem
Minute 4 to 6
Generate structured differentials
Minute 7 to 10
Ask targeted refining questions
Minute 11 to 13
Rank and justify
Minute 14 to 15
Reflect on reasoning and bias
You may adjust timing slightly. The key is maintaining the sequence.
Let us break this down step by step.
Step 1: Define the Core Clinical Problem
Minute 1 to 3
Before thinking about diagnoses, pause and restate the problem in one clear sentence.
Not just the chief complaint.
But a structured summary that includes:
- Age
- Relevant risk factors
- Duration
- Key associated features
For example:
“52-year-old male with acute onset central chest pain radiating to the left arm for 2 hours, with history of hypertension.”
This forces your brain to organize information before jumping to conclusions.
It prevents immediate anchoring.
This step is small, but powerful. It slows impulsive reasoning and builds clarity.
Step 2: Generate Structured Differentials
Minute 4 to 6
Now, create a differential list.
Not just one diagnosis. At least three to five.
Use structure:
- Life-threatening causes
- Common causes
- Context-specific causes
For chest pain, this might include:
- Acute coronary syndrome
- Pulmonary embolism
- Aortic dissection
- Pneumothorax
- Musculoskeletal pain
At this stage, do not rank them yet.
The goal is breadth, not certainty.
This step strengthens analytical reasoning rather than pure pattern recognition.
Step 3: Ask Targeted Refining Questions
Minute 7 to 10
Now return to the case details.
For each differential, ask:
What finding would increase its likelihood?
What finding would decrease its likelihood?
You are now testing hypotheses rather than searching for confirmation.
For example:
If this were pulmonary embolism, would we expect sudden dyspnea?
If this were aortic dissection, would there be tearing pain or pulse differences?
This transforms passive reading into active diagnostic testing.
Clinical case practice for medical students becomes stronger when each case feels like a reasoning experiment, not a puzzle to solve.
Step 4: Rank and Justify
Minute 11 to 13
Now rank your top three diagnoses.
But do not stop at ranking.
Write one sentence explaining why the top diagnosis is currently leading.
Example:
“Acute coronary syndrome is most likely due to typical radiation pattern, risk factors, and acute onset.”
The justification is critical. It reveals whether your reasoning is specific or vague.
If your explanation sounds general, your thinking likely is too.
Step 5: Reflect on Reasoning and Bias
Minute 14 to 15
This is the step most students skip.
Ask yourself:
- Did I anchor too early?
- Did I prematurely dismiss alternatives?
- Did one piece of data disproportionately influence my thinking?
Bias awareness is not advanced theory. It is daily discipline.
Even one minute of structured reflection gradually improves cognitive control.
We explore anchoring bias and its impact in detail in our article on anchoring bias in diagnosis for medical students, as it is one of the most common distortions in diagnostic reasoning.
Applying the 15-Minute Framework: A Case Example
Let us apply the framework step by step.
Case
A 24-year-old female presents with acute onset shortness of breath and pleuritic chest pain for one day. She recently returned from a long-distance flight. No prior medical history. Vitals show mild tachycardia.
Minute 1 to 3: Define the Core Clinical Problem
Structured restatement:
“24-year-old female with acute onset pleuritic chest pain and shortness of breath after prolonged immobilization during travel, with tachycardia.”
Already, this summary highlights:
- Young age
- Acute onset
- Risk factor for thrombosis
- Pleuritic nature of pain
Notice that we have not named a diagnosis yet.
This step protects against immediate anchoring.
Minute 4 to 6: Generate Structured Differentials
Organize systematically.
Life-threatening causes
- Pulmonary embolism
- Pneumothorax
Common causes
- Costochondritis
- Viral pleurisy
Context-specific causes
- Anxiety-related hyperventilation
At this stage, we avoid ranking.
The aim is breadth and safety.
Minute 7 to 10: Ask Targeted Refining Questions
Now test each hypothesis.
Pulmonary embolism
- Risk factor present? Yes, prolonged flight
- Tachycardia? Yes
- Sudden onset? Yes
- Hemoptysis? Not mentioned
Pneumothorax
- Sudden onset? Possible
- Reduced breath sounds? Not provided
- Tall, thin body habitus? Not specified
Costochondritis
- Reproducible tenderness? Not mentioned
- Recent strain? Not mentioned
You are now evaluating likelihood based on data rather than intuition alone.
Minute 11 to 13: Rank and Justify
Top diagnosis: Pulmonary embolism
Justification:
“Most likely due to acute pleuritic chest pain, tachycardia, and recent prolonged immobilization, which is a known risk factor for venous thromboembolism.”
Second: Pneumothorax
Third: Costochondritis
The justification forces specificity.
Minute 14 to 15: Reflect on Reasoning and Bias
Ask:
Did the recent flight immediately anchor me toward pulmonary embolism?
Did I adequately consider pneumothorax despite limited data?
Am I overvaluing one risk factor?
Even if pulmonary embolism remains most likely, the act of questioning strengthens cognitive flexibility.
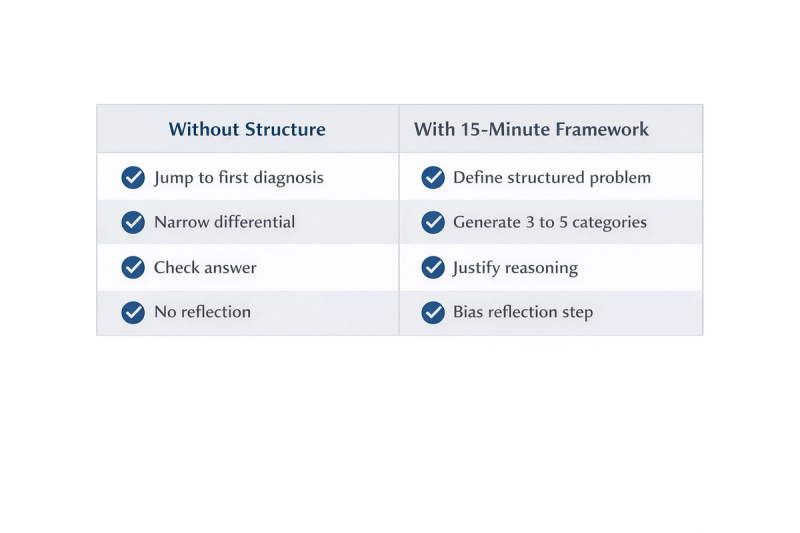
What Changed Compared to Random Solving?
Without structure, the case might have unfolded like this:
Shortness of breath after flight → Pulmonary embolism → Check answer → Correct → Move on
With structure:
- Multiple differentials generated
- Each tested deliberately
- Ranking justified
- Bias reflected upon
The final diagnosis may be the same.
The reasoning depth is not.
This difference compounds over time.
How This Framework Builds Long-Term Diagnostic Thinking
Clinical reasoning does not improve dramatically in a week.
It improves quietly.
When you repeat a structured process daily, three long-term shifts begin to happen.
1. From Guessing to Justifying
Early in training, many diagnoses feel intuitive. You sense what is likely, but explaining why can be difficult.
By ranking and justifying your differentials every day, you train your brain to move from impression to explanation.
Over months, this builds diagnostic confidence that is not dependent on memorization alone.
2. From Pattern Recognition to Analytical Balance
Pattern recognition is valuable. It allows quick identification of common presentations.
However, disciplined clinical case practice for medical students ensures that intuition is balanced with analysis.
You learn to ask:
What else could this be?
What data would change my mind?
This balance becomes especially important when cases are atypical or incomplete, which is common in real clinical settings.
3. From Isolated Thinking to Collaborative Refinement
Clinical reasoning develops faster when it is discussed.
When you explain your differential to a peer and they ask, “Why not this diagnosis?” your thinking becomes sharper. Gaps become visible. Blind spots become easier to identify.
This is one reason structured case discussion matters.
A framework gives everyone a shared language. When students approach cases with similar structure, discussion becomes clearer and more productive. Instead of debating conclusions, the conversation focuses on reasoning pathways.
That is the culture Medcoterie aims to support. A space where clinical case practice for medical students is not just individual effort, but collaborative refinement. Not competitive answer sharing, but structured reasoning exchange.
The goal is not to prove who is right first.
The goal is to understand how each person reached their conclusion.
Consistency Over Intensity
One structured case per day is enough.
Not because volume is unimportant.
But because consistency builds cognitive discipline.
If practiced regularly:
- Your differentials become broader
- Your ranking becomes clearer
- Your bias awareness becomes sharper
- Your discussions become more precise
Clinical reasoning becomes less reactive and more deliberate.
This gradual shift is what ultimately prepares you for real patient encounters, where uncertainty is common and decisions carry weight.
Building a Sustainable Habit of Clinical Case Practice
Return to the student from the beginning.
The case was correct.
The reasoning felt uncertain.
Now imagine the same student approaching one case each day with structure.
Restating the problem clearly.
Generating structured differentials.
Testing each possibility deliberately.
Ranking with justification.
Reflecting briefly on bias.
Nothing dramatic changes overnight.
But after weeks, something subtle shifts.
The differential lists become broader.
The explanations become clearer.
Discussions with peers become sharper.
Confidence starts to come not from recognizing patterns alone, but from understanding the pathway of reasoning.
Clinical case practice for medical students does not need to be intense. It needs to be consistent and structured.
One well-analyzed case daily is more transformative than multiple cases solved without reflection.
Over time, this structure becomes internal. You no longer consciously follow each step. The reasoning process becomes organized by habit.
And when that reasoning is discussed openly, refined collaboratively, and questioned respectfully, it strengthens further.
That is the culture Medcoterie seeks to support. A space where clinical case practice is not competitive answer sharing, but thoughtful diagnostic dialogue. Where students are comfortable saying, “This was my reasoning. What did I miss?”
Clinical reasoning develops slowly. It develops through repetition, reflection, and conversation.
The 15-minute framework is simply a starting structure.
The growth comes from how consistently and collaboratively it is practiced.
References:
1. National Academies of Sciences, Engineering, and Medicine
Improving Diagnosis in Health Care (2015)
Landmark report on diagnostic error and clinical reasoning.
https://nap.nationalacademies.org/catalog/21794/improving-diagnosis-in-health-care
2. Croskerry P.
The importance of cognitive errors in diagnosis and strategies to minimize them.
Academic Medicine. 2003;78(8):775–780.
https://journals.lww.com/academicmedicine/Fulltext/2003/08000/The_Importance_of_Cognitive_Errors_in_Diagnosis.3.aspx
3. Eva KW.
What every teacher needs to know about clinical reasoning.
Medical Education. 2005;39(1):98–106.
https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2929.2004.01972.x
4. Norman G.
Dual processing and diagnostic errors.
Advances in Health Sciences Education. 2009;14(Suppl 1):37–49.
https://link.springer.com/article/10.1007/s10459-009-9179-x
5. Graber ML, Franklin N, Gordon R.
Diagnostic Error in Internal Medicine.
Archives of Internal Medicine. 2005;165(13):1493–1499.
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/486778