Anchoring bias in diagnosis: what it looks like on the ward as an intern

Anchoring bias in diagnosis is one of the most common reasoning errors in intern ward work, and it is almost never visible from the inside when it is happening. It happens when your first clinical impression becomes fixed before the case has been properly evaluated.
For most interns, the anchor does not form at the bedside. It forms through the admitting diagnosis written at the top of the chart, or through the first two lines of the case summary. By the time you are standing in front of the patient, the reasoning has already begun to narrow around that first label.
Anchoring bias in intern-level clinical reasoning almost always enters through the admitting diagnosis, not through the physical examination.
Why does anchoring feel like clarity on the ward?
The answer that comes first does not feel like a guess. It feels like recognition. You hear the history, something matches a pattern you have seen before, and there is a distinct sense of relief. That relief is the problem.
On the ward, especially in the first posting, relief is something you are quietly starved of. Everything is uncertain. The consultant is waiting. The patient is looking at you. The first coherent diagnosis is not just a clinical hypothesis. It is a foothold. And once you are holding it, you stop looking for another place to stand.
This is not a failure of intelligence. It is how pattern recognition works before it is disciplined by experience. Experienced clinicians anchor too, but they have enough variation in their exposure to know which patterns break down and when. As an intern in your first medicine or surgery posting, you are working with a much smaller set of reference cases. The first familiar explanation is also the most persuasive one, because it is often the only one you have seen in practice rather than only in a textbook.
What does anchoring actually look like during a ward case?
It is easier to see in an example than in a definition.
The Initial Presentation
A 52-year-old man presents to casualty with central chest pain for two hours. The pain is burning in character and started after a heavy meal. He has a history of hypertension. His ECG shows no acute changes. Vitals are stable.
The first thought in the discussion is gastritis. The pain started after food. It is burning. The ECG is clear. That initial label feels reasonable, and it is not irrational.
What anchoring does to the reasoning from that point
Once gastritis enters the picture, the reasoning stops widening and starts confirming. The burning character of the pain is emphasised. The heavy meal becomes the central clue. The normal ECG becomes reassurance rather than just one data point. Nobody asks out loud what else could explain a two-hour episode of central chest pain in a hypertensive 52-year-old man.
The clues for an atypical presentation of acute coronary syndrome were present. Central location, not clearly epigastric. Two hours without relief. Age and hypertension as risk factors. None of them were hidden. They were simply filtered through the first explanation.
What broke the anchor
A senior asks one question: what if this is not gastritis?
Troponins are ordered. They return elevated. The diagnosis shifts to NSTEMI.
The initial reasoning was not wrong because the students lacked knowledge. It narrowed because the first plausible answer reduced the motivation to keep searching. That is anchoring. Not ignorance. Premature closure.
Why are interns particularly at risk during the first posting?
There is real pressure during ward rounds to present confidently and move quickly. Pausing to say you are still considering alternatives can feel like uncertainty in a setting that does not always reward uncertainty. Speed reads as competence. The intern who names a diagnosis fast and moves to management sounds like someone who knows what they are doing.
That pressure is particularly acute in the first posting, usually medicine or surgery, before you have seen enough variation to know that the textbook presentation is often the exception on the ward. You have studied pneumonia carefully. The three cases you have seen look like the textbook. The fourth one will not, but you will not know that until you see it. Until then, the pattern feels complete.
In Indian teaching hospitals, ward rounds move fast. There are many patients. The consultant is often several beds ahead. The intern who hesitates gets left behind. That structural reality creates conditions where anchoring is not just a cognitive tendency. It is a response to the environment.
Knowing this does not fix it. But it changes how you approach your own reasoning. The problem is not that you anchor. The problem is anchoring without knowing you have.
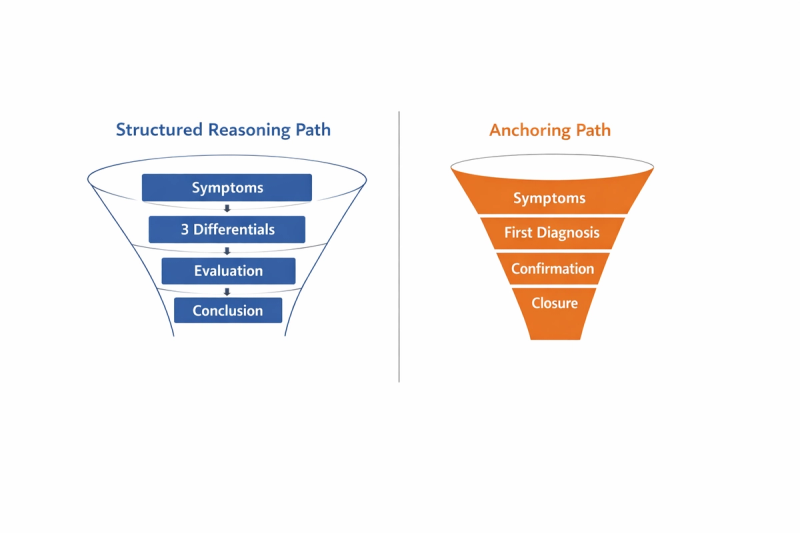
How do you interrupt anchoring bias before it closes the case?
The goal is not to distrust your first impression. It is to prevent it from becoming final before the reasoning has properly opened.
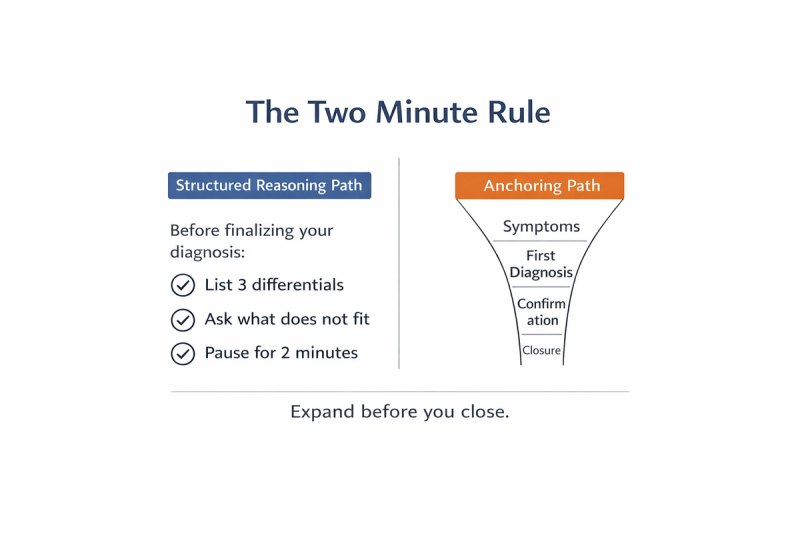
Name three differentials before you narrow to one
Even when the diagnosis feels obvious, write down three alternatives before committing. They do not need to be equally likely. The purpose is not balance. It is to force the reasoning to stay open for one more moment before closing. Anchoring is automatic. The list is deliberate.
Ask what does not fit
After your first hypothesis, spend thirty seconds looking for one feature that does not align. Is the timeline slightly off? Is a risk factor missing? Is there a symptom that the diagnosis does not account for cleanly? You do not need to find a contradiction. You need to look for one. The search itself interrupts the narrowing.
Return to the history after the examination
Anchoring often happens before the physical examination is complete. The hypothesis forms from the history, and then the examination is conducted inside that frame. Going back to the history after you have examined the patient, before you present, gives you a second pass that is not shaped by the first impression in the same way.
Use the question your senior used
Before you close the case, ask yourself once: what if this is wrong? Not because it probably is. Because the question itself creates a pause between your first impression and your final conclusion. That pause is where the reasoning either widens or confirms prematurely.
If you practice cases with a batch or in a peer space, surfacing differentials together naturally exposes anchors that are harder to see alone. When someone else asks what else could this be, it is easier to hear than when you ask it yourself.
A Simple Cognitive Habit That Prevents Anchoring Bias
If you build a habit around a simple, time bound reasoning routine, such as the approach outlined in How to Practice Clinical Cases Daily as a Medical Student: A Structured 15-Minute Framework, anchoring becomes less likely without requiring constant self correction.. The structure itself slows premature certainty.
Peer discussion strengthens this further. When reasoning is shared out loud rather than simply declared, anchors that are invisible to you become visible to someone else. A batchmate who asks what else could this be is not challenging your diagnosis. They are doing the thing the structure is supposed to do. This is what MedCoterie is built for: not a space to present confident diagnoses, but a space to think through uncertain ones, where surfacing an alternative is the norm rather than the exception
The first posting is where most reasoning habits quietly form. Not in the textbook. Not in the OSCE. In the moments between the admitting note and the ward round, when you are standing with a case in front of you and no one is watching how you think. The gap between the first answer that feels right and the last alternative you considered is where clinical reasoning either develops or stops. You are already inside that gap.
References
- Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them. Academic Medicine. 2003;78(8):775–780.
- Croskerry P. Diagnostic failure: A cognitive and affective approach. In: Advances in Patient Safety: From Research to Implementation. Vol 2. Rockville, MD: Agency for Healthcare Research and Quality; 2005.
- Graber ML, Franklin N, Gordon R. Diagnostic error in internal medicine. Archives of Internal Medicine. 2005;165(13):1493–1499.
- National Academies of Sciences, Engineering, and Medicine. Improving Diagnosis in Health Care. Washington, DC: The National Academies Press; 2015.
- Norman G, Monteiro S, Sherbino J. Is clinical cognition binary or continuous? Advances in Health Sciences Education. 2013;18(3):435–446.