Clinical reasoning errors interns make in the first posting: 7 patterns to recognize early

If you are in your first medicine or surgery posting and your reasoning feels broken, you are not behind. You are in the phase where patterns form -- and the ones forming right now will shape how you think about every patient for the next decade.
Clinical reasoning errors in interns almost never come from not knowing enough. They come from how we are thinking, and seven patterns show up again and again in the first posting, usually without the intern realizing it.
The reasoning errors that follow interns into their careers are not formed in final year MBBS, they are formed in the first posting, when thinking under pressure becomes a habit before anyone has named what that habit is.
Why the first posting is when reasoning habits actually form
In the first weeks of your medicine or surgery posting, the pressure is constant. The ward round moves fast. The consultant does not stop to explain. You present the patient, someone corrects you, and you move on. There is no time to audit your thinking.
This is exactly when reasoning shortcuts become automatic. The brain finds the fastest path that worked last time and uses it again. If the shortcut is anchoring too early, or closing the case before exploring alternatives, it does not just affect today's presentation. It becomes the default response next week, and the week after.
This is why recognising these patterns in week 3 of your first posting matters more than recognising them in year 3 of residency. Named early, they are easy to interrupt. Unnamed, they compound quietly into something much harder to shift.
7 reasoning patterns that form in the first posting
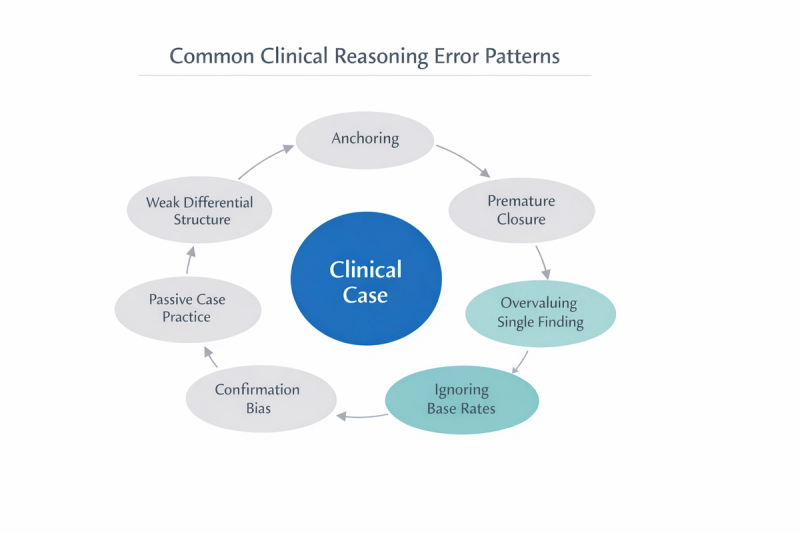
Error 1: Anchoring on the First Diagnosis That Fits
This is the most common error in the first posting, and the most invisible. A patient presents with fever, productive cough, and crackles on auscultation. You think pneumonia. From that moment, everything else gets filtered to support that idea. Weight loss, longer duration, night sweats - these details get quietly downplayed instead of widening the differential toward tuberculosis or malignancy.
Anchoring does not happen because you are careless. It happens because the ward round is moving and your brain wants certainty. On the post-round, the feeling that you had the right answer from the start is comfortable. But if you anchored, you were not reasoning, you were confirming.
How to interrupt it on the ward:
- After forming your first impression, stop and ask: what would make this diagnosis wrong?
- Force yourself to name two alternative diagnoses before presenting. Even if you still conclude the first is correct, the act of building alternatives keeps your reasoning open.
Error 2 -- Premature closure before exploring what you might have missed
Premature closure is different from anchoring. Anchoring is attaching to the first idea. Premature closure is stopping the thinking process too early, usually the moment the case feels solved.
A young patient in the casualty presents with chest pain that worsens on breathing. You think costochondritis, the presentation fits, and you close the case in your mind. But pulmonary embolism, pneumothorax, and pericarditis all need to be briefly considered and set aside deliberately, not bypassed because the first answer felt sufficient.
On a busy medicine ward in the first posting, efficiency feels like a virtue. But closing a case before asking 'what is the serious thing I must not miss' is not efficiency, it is a gap in the process.
How to interrupt it on the ward:
- After stating your working diagnosis, add one step: name the most serious alternative that must be ruled out.
- This habit does not slow you down significantly. It trains your brain to keep the case open until it has genuinely been closed.
Error 3: Overvaluing a Single Finding and letting it dominate the case
A patient comes in with fatigue, pallor, and mild breathlessness. The haemoglobin is low. You immediately focus there, iron deficiency anaemia and the lymphadenopathy in the neck gets noted but not weighted appropriately. The peripheral smear is ordered but not reviewed with the same attention.
One abnormal value feels like a focal point, and focal points are comforting on a ward where everything else feels uncertain. But clinical reasoning is pattern recognition across multiple findings. When one finding dominates, the others fade and that is where the gaps appear.
How to interrupt it on the ward:
- After identifying the key finding, deliberately ask: what else in this case does not fully fit this explanation?
- If two or three elements seem inconsistent, that is a signal to widen the differential, not narrow it.
Error 4: Ignoring Base Rates and Common Diagnoses
In the first posting, rare presentations feel memorable. You have read about them, discussed them in case presentations, heard them mentioned by consultants. Over time, this quietly distorts how you estimate probability.
A young patient presents with headache and vomiting. You have been reading neurology recently and begin building a detailed intracranial differential. But in a busy outpatient setting, tension headache, migraine, and viral illness account for the vast majority of presentations with this pattern. Building a rare differential first, without first accounting for common causes, is not thoroughness. It is an uncalibrated estimate.
Base rates matter most in the first posting, where clinical exposure is new and memorable cases from textbooks crowd out probabilistic thinking.
How to interrupt it on the ward:
- Before finalizing your differential, ask: what is the most common explanation for this presentation in this age group and setting?
- Then justify, clearly, why you are moving past it, if you are.
Error 5: Confirmation Bias During Case Presentation
Confirmation bias is the quietest error on this list. You are not inventing findings. You are filtering them. The details that support your diagnosis feel important. The details that do not fit get noted but not weighted.
A patient with a history of alcohol use presents with epigastric pain. You suspect acute gastritis and present accordingly. The mild jaundice that appeared in the notes, and the slightly enlarged liver on examination, get mentioned but not connected, because they complicate a diagnosis that already feels settled.
The ward round does not always create space to say 'I am not sure.' Confirmation bias fills that space with something that feels certain but is actually selective.
How to interrupt it on the ward:
- After presenting your diagnosis, name one finding that argues against it.
- If you genuinely cannot find one, the case may not have been examined critically enough.
Error 6: Weak Structuring of the Differential Diagnosis
Most interns can produce a differential list in the first posting. What is harder is organising it in a way that shows reasoning rather than recall.
Saying 'pneumonia, tuberculosis, lung cancer, pulmonary embolism' is a list. It is not a differential. A structured differential groups possibilities by mechanism, urgency, or category, and it shows the examiner, the consultant, and yourself that you have thought through the case rather than retrieved a list from memory.
Unstructured differentials are common in the first posting because the pressure is on naming things, not organising them. But an organised differential is the difference between looking like you are thinking and actually thinking.
How to interrupt it on the ward:
- Group your differentials into categories: infectious, inflammatory, malignant, vascular, or whatever fits the system.
- Present the most immediately dangerous possibility first, even if it is less likely, then move to the most probable.
Error 7: Passive Case Practice Instead of Active Reasoning
In the first posting, you see cases every day. You watch consultants reason through them. You sit in case discussions and hear the correct diagnosis explained. This feels like learning, and some of it is. But watching someone else reason is not the same as reasoning yourself.
The difference shows up when you present a case on your own for the first time. The differential that seemed obvious in the case discussion is no longer obvious when you have to generate it under pressure.
Passive exposure builds familiarity. Active reasoning builds the actual skill.
How to interrupt it on the ward:
- Before reviewing any case explanation or answer, write down your working diagnosis, your key differentials, and your reasoning.
- Only then compare. The gap between what you thought and what was correct is where the learning actually lives.
How to Turn These Errors Into a Daily Improvement System
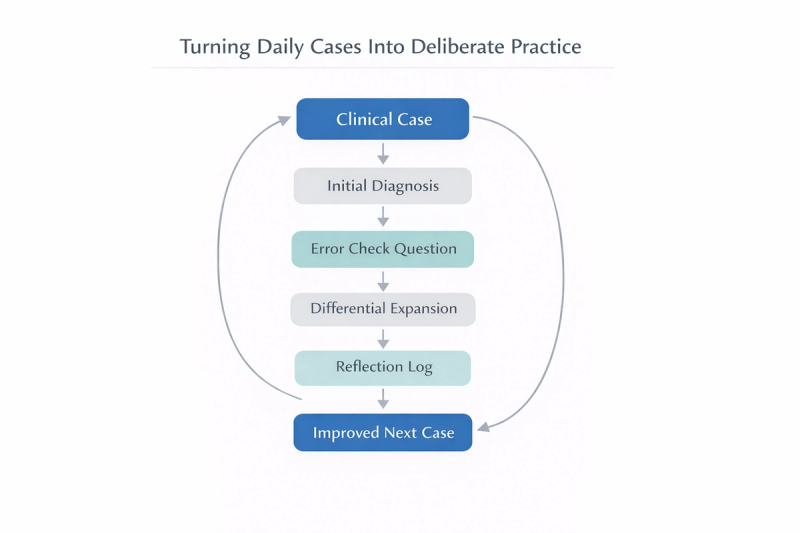
Recognizing these seven errors is the first step. Using them during the posting is where they become useful.
At the end of each case, whether it is a ward round presentation, a casualty admission, or a case discussion with your batch, ask one question instead of 'did I get it right':
What reasoning error did I almost make today?
Keeping a brief note of which patterns appear most often across a week tells you more about your reasoning than any case presentation score. If you anchor frequently, you know where to interrupt. If you close cases too early, you know which question to add to your routine.
These patterns are not failures. They are the predictable output of a brain learning to reason clinically under pressure, with incomplete information, in a hierarchy that does not always make it safe to say you are uncertain. Every intern in every first posting is working through some version of these seven patterns right now.
The difference between an intern who improves quickly and one who does not is usually not knowledge. It is whether they are watching their own reasoning or just watching the clock.
A 15-minute structured case routine makes it easier to integrate bias awareness directly into your workflow rather than treating it as an abstract concept.
This is what MedCoterie is for - not catching each other's errors, but naming them together, in a space where not knowing is the starting point, not the embarrassment.
The first posting is where you are learning to think like a clinician while simultaneously learning where everything is, what to say on the ward round, how to talk to patients, and how to function inside a hierarchy that gives you almost no room to say you do not know. The reasoning errors are not the sign that something has gone wrong. They are the sign that the thinking is happening, just not yet with enough structure to catch itself. That comes with time, and with the habit of looking.
References
- Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them. Acad Med. 2003;78(8):775–780.
- Graber ML, Franklin N, Gordon R. Diagnostic error in internal medicine. Arch Intern Med. 2005;165(13):1493–1499.
- Norman G, Eva K. Diagnostic error and clinical reasoning. Med Educ. 2010;44(1):94–100.
- Kahneman D. Thinking, Fast and Slow. Farrar, Straus and Giroux; 2011.
- Ericsson KA. Deliberate practice and acquisition of expert performance. Acad Emerg Med. 2008;15(11):988–994.